Latest News
Alternative Dispute Resolution in Health Care

Alternative Dispute Resolution in Health Care
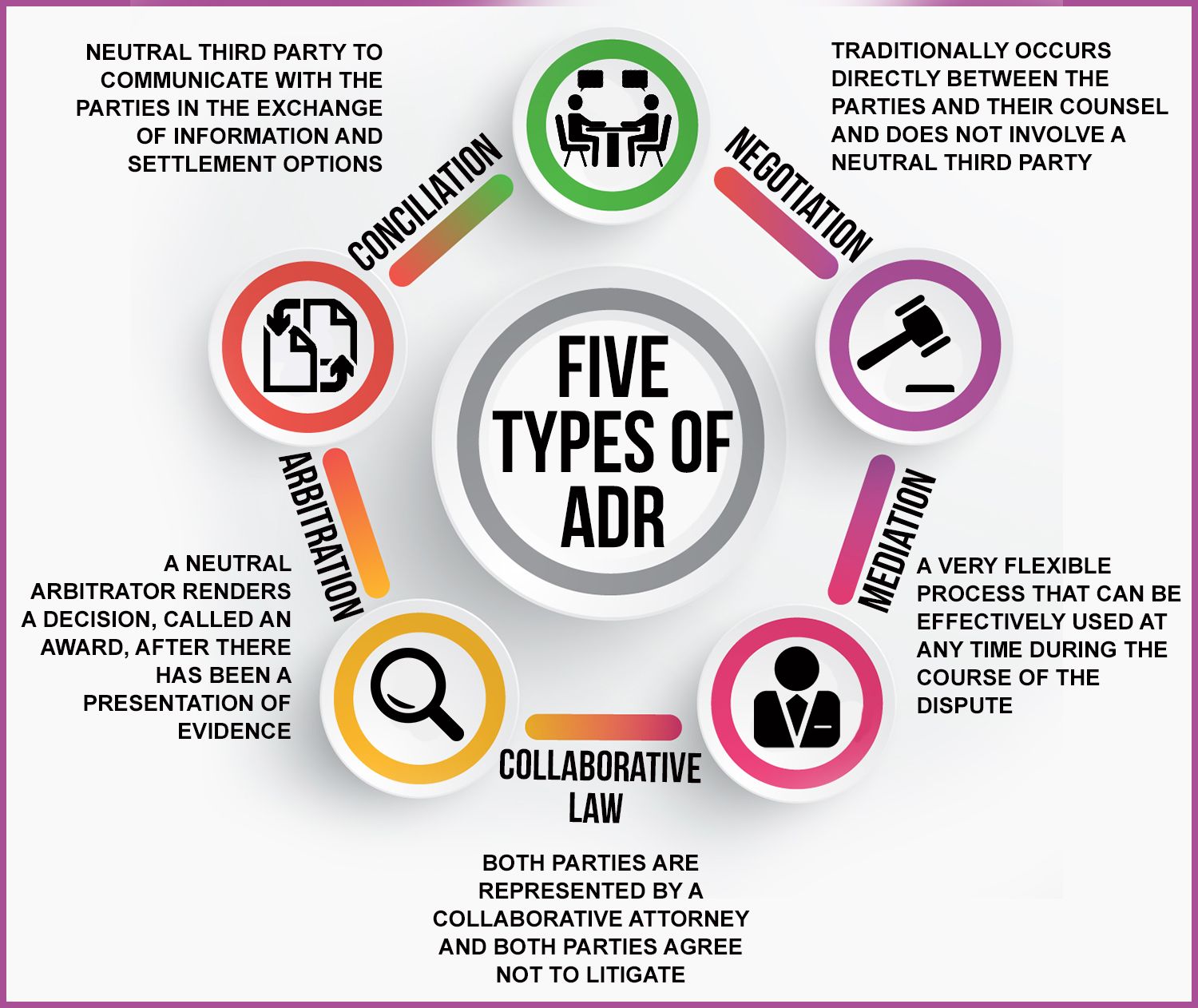
For ages, medical malpractice and the misbehaviors of the people in the industry have been one of the main conventional conflict points that pertain to dispute resolution in matters related to the delivery of healthcare. In the past few years, the managed care concept has increased rapidly, therefore the possibilities of disagreements, which have frequently increased state reforms and the development of alternative dispute resolution mechanisms and procedures. The requirement for effective, equitable, and undamaged disputant interactions has also grown with the extension of managed care as the patients and plan subscribers of that particular medical institution have been asked more and more by doctors, hospitals, and health plan consignment takers to consent and sign the binding arbitration clause of any complaints.
Arbitration agreements are binding, and they are also required in the supply of healthcare. They come in the form of clauses inserted into contracts between health plans and their buyers and enrollees, as well as particular agreements given to patients by hospitals and doctors at the beginning of their association. These agreements include a broad outline of the rules controlling the process and mandate that binding arbitration be used to settle any future disputes between the parties. The parties hereto expressly and irrevocably relinquish all claim to a trial or judicial review of their disputes. The argument that arbitration is better than the courts for several reasons, including efficiency, consistent, informed decision-making, preservation of significant relationships, claimant satisfaction, confidentiality, forfeiture of the right to appeal, and loss of precedent, is becoming more and more prevalent in the discussion surrounding the effects of legally binding arbitration agreements.[1] Legislators and the courts are now being urged to weigh in on the worth and suitability of these agreements, especially about the provision of healthcare.
A reasonable consensus on dispute outcomes, such as caseload characteristics, time to disposition, transaction costs, patterns of awards and settlements, disputant perceptions of fairness and satisfaction, and neutral quality, is suggested by evaluating alternative dispute resolution (ADR) programs currently in place. The majority of published research, however, focuses on the outcomes of non-binding, court-mandated arbitration programs that are implemented as a part of several court reform and tort reform packages, which raises questions about the validity of the study's results. There are few empirical assessments of the effects of private, binding arbitration, and those that exist suffer greatly from their eclectic and ambiguous evaluation methods, tiny arbitrated caseloads, and sometimes questionable comparator groups. Although these programs do not greatly decrease trial rates, disputants are consistently very satisfied with both the procedure and the result. Determining private, binding arbitration is considerably more challenging since the information required for a comprehensive, non-proprietary assessment is widely scattered, confidential, and sometimes well-guarded. This research looks at how arbitration agreements are used in the healthcare system and discovers that private, legally binding arbitration of medical issues is uncommon.[2]
References
[1] Rolph, Elizabeth, Erik Moller, and John E. Rolph. "Arbitration Agreements in Health Care: Myths and Reality." Law and Contemp. Probs. 60 (1997): 153.
[2] Rohlik, Josef. "Arbitration as a Model for Resolution of Health Care Disputes Between Health Care Professionals and Health Care Organizations.". Louis ULJ 41 (1996): 1005.
- he healthcare sector is increasingly utilizing arbitration agreements, requiring patients to consent to binding arbitration clauses, especially within managed care.
- Benefits of binding arbitration, such as efficiency and confidentiality, are acknowledged.
- Empirical assessments on private, binding arbitration in healthcare are lacking.